Facial Plastic Surgery

Dr. Kahana and the team at Kahana Oculoplastic Surgery specialize in cosmetic surgeries and procedures for facial rejuvenation with a focus on the eyelids, forehead and midface.
A cosmetic bitemporal brow lift is a surgical procedure that specifically targets the outer or lateral aspect of the brows.
This technique is used to correct drooping of the outer aspect of the brows, which can contribute to a tired, melancholy, or sad facial expression.
This surgery is often performed under local anesthesia with sedation. The surgeon makes an incision along the forehead, next to the hairline, which allows for concealment of the incision sites. Next, the brow tissue is elevated and repositioned for the desired results. This procedure can help achieve a more youthful and refreshed appearance while maintaining a natural look.

A cosmetic forehead lift, also known as a complete brow lift, is a surgical procedure that aims to lift and rejuvenate the upper aspect of the face.
This procedure involves lifting and tightening the skin and underlying muscles of the forehead to smoothen out the forehead wrinkles and frown lines between the eyebrows and raise the eyebrows.
There are different types of forehead lifts, including a classic or coronal forehead lift, an endoscopic forehead lift, and trichophytic forehead lift. The type of forehead lift best suited for each person is different and is based on each person’s unique existing anatomy and desired outcomes. This type of surgery may be combined with a facelift.
A forehead lift is often performed under local anesthesia with sedation. The recovery time varies depending on the extent of the surgery and the individual’s healing process.
This procedure results in a more rejuvenated, alert, and refreshed appearance while maintaining a natural and harmonious lift.


A cosmetic facelift, also known as a rhytidectomy, is a surgical restorative procedure that aims to lift and rejuvenate the lower aspect of the face.
This procedure involves lifting and tightening the excess skin along the face to address signs of aging, such as wrinkles, jowls, and sagging skin. The goal is to attain a naturally youthful facial appearance.
A facelift is a type of surgery that may be performed with sedation and local anesthesia or with general anesthesia. This type of procedure may be combined with a forehead lift.

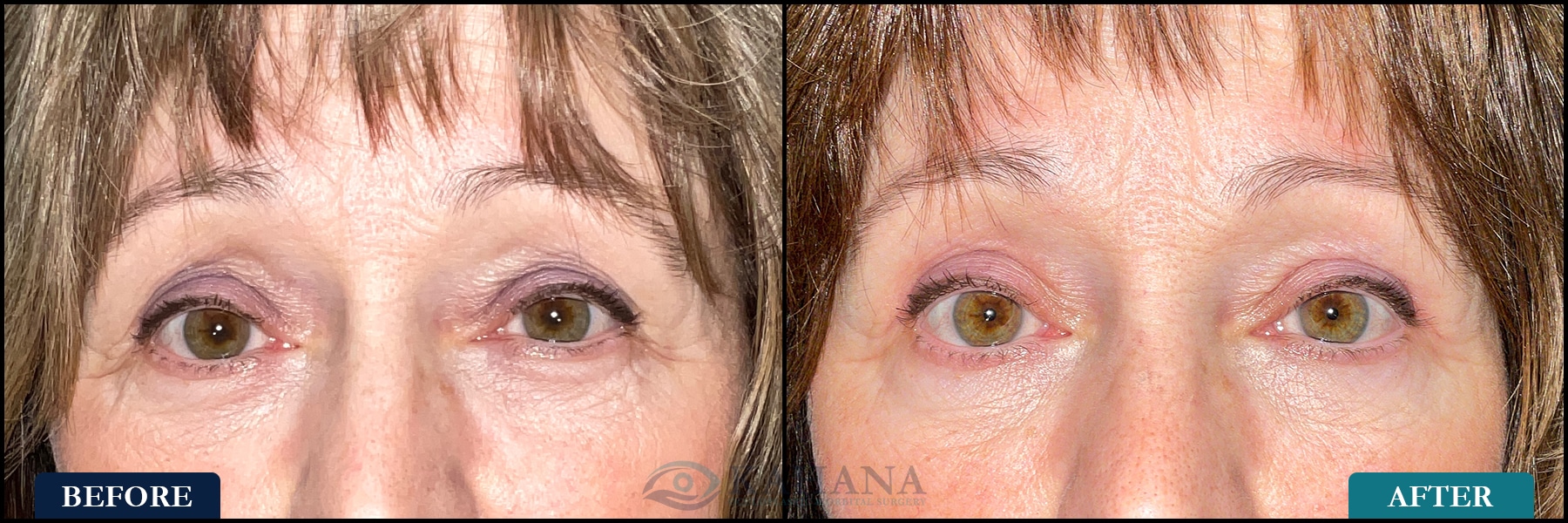
Cosmetic upper eyelid blepharoplasty (also referred to as an “eyelid lift”) is a surgical procedure designed to rejuvenate the appearance of the eyes by removing excess skin and sometimes fat from the upper eyelids.
This popular aesthetic surgery addresses issues such as drooping eyelids and puffy, baggy eyelids that contribute to a tired or aged appearance.
The procedure involves making precise incisions along the natural crease of the upper eyelids, allowing for the discreet removal or repositioning of tissue. This not only results in a more alert and youthful look but can also improve peripheral vision obstructed by overhanging skin. The surgery is typically performed under local anesthesia, often with mild sedation, and is known for its relatively rapid recovery period.
Blepharoplasty can be tailored to meet the individual’s aesthetic goals, taking into account factors like skin type, ethnic background, and overall facial structure.
The outcome is a refreshed and rejuvenated appearance, with scars usually well-concealed in the eyelid crease. This procedure is popular among both men and women seeking to reduce signs of aging around the eyes and enhance their overall facial appearance.


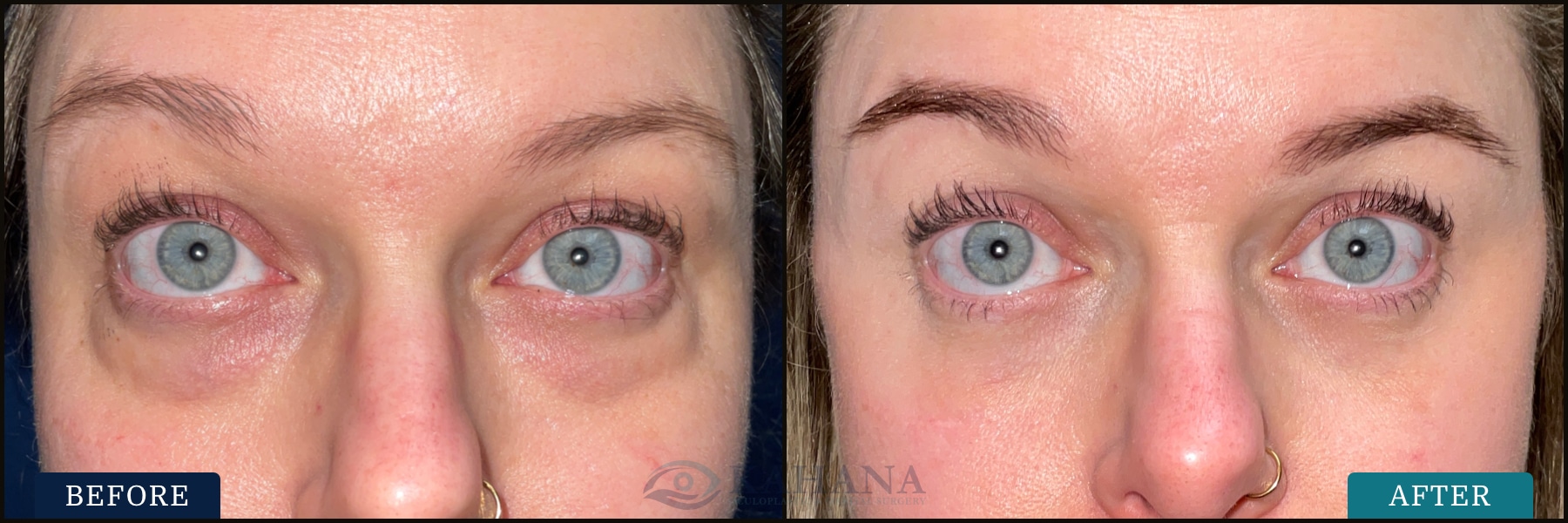
Cosmetic lower eyelid blepharoplasty is a surgical procedure aimed at rejuvenating the area under the eyes by addressing issues like under-eye bags, wrinkles, and sagging skin.
This procedure typically involves the removal or repositioning of fat, along with the excision of excess skin and tightening of the underlying muscles, to create a smoother, more youthful appearance.
The incisions are strategically placed just below the lash line or inside the eyelid (transconjunctival approach) to minimize visible scarring. This technique is particularly effective for correcting puffiness and dark circles that give a tired or aged look.
It’s a popular choice for individuals seeking to rectify the effects of aging, hereditary factors, or lifestyle influences that contribute to a worn-out appearance under the eyes.
Lower eyelid blepharoplasty is often performed under local anesthesia with sedation, and the recovery time varies depending on the extent of the surgery and the individual’s healing process. The result is a refreshed and revitalized eye area, enhancing the overall facial aesthetics and often boosting the patient’s self-confidence.

Asian eyelid surgery, or double eyelid surgery, is a type of upper eyelid blepharoplasty procedure that creates an upper eyelid crease.
This procedure is designed to enhance the upper eyelid in patients who have a natural “monolid” or single eyelid without a crease. This normal anatomic variation is most commonly seen in individuals of East Asian descent (i.e., China, Korea, Mongolia, Japan, and Hong Kong), and is the result of how the subcutaneous tissue attaches to the overlying upper eyelid skin.
With Asian eyelid surgery, the height of the new eyelid crease is customized based on the patient’s unique eyelid structures and existing anatomy, as well as the desired outcome.
It’s important that the surgeon has a thorough understanding of each patient’s aesthetic goals and unique anatomy to achieve results that are both natural and harmonious with the patient’s overall facial features.
Eyelid crease revision is a surgical procedure aimed at augmenting a person’s natural eyelid crease or correcting the results of a previous eyelid surgery.
This procedure involves adjusting the position, depth, shape, or contour of the eyelid to achieve a more desirable and aesthetic look.
This often requires meticulous surgical precision and a careful understanding of the patient’s existing eyelid anatomy and desired outcome.
We also offer a wide range of non-surgical procedures, including CO2 laser resurfacing, Botox, iLux, and more.
The team at Kahana Oculoplastic Surgery specializes in facial rejuvenation procedures with a focus on the eyelids, forehead and midface.